Q. What is Obesity?
Obesity refers to an excess of body fat. The term overweight means an excess weight for the height and when the weight excess is enormous, it is termed obesity.
Q. How do I know if my child is overweight or obese?
A more scientific way of assessing this is by calculating the Body Mass Index (BMI).
Body mass Index = Weight in kilograms / Height in m2
If you know your child’s height and weight, you can calculate the body mass index by using the BMI calculator given. You can plot the BMI against the age on the specific chart for boys or girls.
If Your BMI is within:
- -50th percentile, it is normal
- -85th to 95th percentile, it is considered to be overweight
- -Greater than the 95th percentile, it is considered to be obese
Children who are overweight or obese should be investigated by their pediatric endocrinologist for abnormalities that may have caused the obesity or resulted from obesity.
Calculate your BMI here.
Q. What is the reason for my child being overweight?
Deposition of fat in the body and weight gain occurs when you are taking more calories (eating large amounts of food or more fatty foods) or utilizing less calories ( by physical activity) or both.
You do find some children and adolescents eating almost the same food and exercising the same amount, one may be overweight and the other may seem normal. This is because genetic factors also govern the amount of weight gain. Some people seem to gain weight more easily than others and have to watch what they eat.
Occasionally excess weight gain may be due to an under-active thyroid gland or overactive adrenal gland and rarely it may be due to marked increase in appetite secondary to certain genetic syndromes or tumors.
Q. What are the effects of being overweight?
The effects of obesity depend on the degree of excess weight or BMI. The higher the BMI, the greater is the risk of these children or adolescents becoming obese adults and developing diseases such as diabetes mellitus, hypertension, abnormalities of the lipid profile and coronary (heart) disease later in life. If there is a history of these illnesses in the family, then the risk is even higher.
In the last few years there has been a marked increase in the development of diabetes in adolescents and it has almost become an epidemic in the developed countries. Even in a developing country like India a marked increase in obesity has been observed in the last few years, although official statistics are limited. There has also been an increase in the number of children who are developing diabetes, hypertension and abnormalities of the lipid profile in our population since the Indian population is genetically at a very high risk of developing these diseases.
These children may also develop problems of the joints due to excess weight bearing. Females may develop abnormalities in their menstrual periods and excessive hair on the face etc. due to the effect of obesity on hormones. Besides the risk of developing complications, cosmetic problems also affect these young children and may cause psychosocial problems.
Q. Does Lifestyle have an effect on weight gain?
The epidemic of obesity is primarily due to the change in lifestyle.The availability of high fat foods (fast food) is a big temptation for children. Lack of physical activity is rampant because of increased TV viewing & spending time in front of computers. Even in schools the time allotted for physical activity has reduced in the last few years and the pressure of studies has contributed to a relatively sedentary lifestyle for young children and adolescents.
Q. How do I get my child to lose weight?
Management in children and adolescent is aimed at controlling the weight gain so that as the child gains height, the weight will get adjusted. A gradual weight loss may be required in those who have completed their growth or are grossly obese.
Avoiding calorie dense foods with high fat content and physical exercise to burn calories form the basis of weight loss. Rapid weight loss or severe dietary restriction is not recommended since good nutrition is required for growth in children and adolescents. The whole family should be involved in weight management and should help in the modification of lifestyle.
Weight management should be done under the supervision of your endocrinologist.
Q. Can I prevent my child from becoming obese?
Yes, you can prevent your child from becoming obese. Preventing obesity is more important and much easier than treating it. Regular monitoring of height and weight by your pediatrician will help to identify those who are gaining excess weight, so this can be prevented before the child becomes obese.
Teaching healthy behaviors at a young age is important since change becomes more difficult with age. Behaviors involving physical activity and nutrition are the cornerstone of preventing obesity in children and adolescents. Families and schools are the two most critical links in providing the foundation for those behaviors.
Q. What is puberty?
Puberty is the stage in a child’s life during which he or she matures physically (sexually) and becomes an adult. eg.
- - Breast development in girls,
- - Increase in the size of the testes in boys,
- - Appearance of hair in the pubic area and underarms for both.
Q. How does puberty occur?
Puberty starts under the influence of hormones secreted by the pituitary gland, which is a small gland present in the brain. The gland gets active between 8-13 years in girls and 9-14 years in boys. It produces 2 hormones called LH and FSH. These 2 hormones act on the ovaries in girls and testes in boys. The ovaries start producing the female hormone estrogen in response to the LH and FSH, which results in breast development, enlargement of the uterus and results in menstruation( periods ) after 1-2 years.
The testes in boys start enlarging in response to the pituitary hormones and secrete a hormone called testosterone. Testosterone results in the appearance of sexual hair, enlargement of the penis, deepening of voice and facial hair.
The appearance of hair in the pubic and axillary area and the penile enlargement are controlled by another gland called the adrenal glands that are located above the kidneys. These glands produce certain hormones called the DHEA,17a(OH)progesterone and Testosterone, which are responsible for appearance of sexual hair. This has been termed as adrenarche (activation of adrenal glands)
Q. At what age should these changes occur in a child?
These changes in the body typically start at an average of 11 years in girls and 12 years in boys.
Q. What is early/precocious puberty and what are the symptoms?
Early puberty is the:
- - Development of breasts and hair in the pubic and underarm area before the age of 8 years in girls
- - An increase in the size of the testes or hair in the pubic and underarm area before 9 years in boys.
Q. Is early puberty common?
Early puberty is more common in girls compared to boys, although boys can also develop this problem.
Q. Do I need to consult a doctor for this?
Yes, it is very important for you to get in touch with your pediatrician or a pediatric endocrinologist if you notice
- - Breast development or sexual hair before 8 years in girls or
- - If girls have periods before the age of 9-10 years and
- - If boys have sexual hair or an increase in the size of the testes or size of the penis before 9 years of age. A specialist would be needed to measure the size of the testes in boys with a special instrument called the orchidometer to confirm the increase in size.
Seeing signs of early puberty in your child can be worrisome, but don’t worry. It is treatable.
Q. What are the common causes of early/precocious puberty?
In most cases of girls with precocious puberty, the cause is unknown. In girls with signs of puberty before 6 years and in all boys, early puberty could be due to an abnormality of the pituitary gland. An MRI may be needed to look for an abnormality in the pituitary gland.
Occasionally girls could get breast development due to a cyst in the ovary. Early appearance of hair in the pubic or underarm area in girls and boys could be due to an abnormality of the adrenal gland. This can also cause an enlargement of the penis in boys and the clitoris in girls
Q. What are the effects of precocious puberty
Most children who begin puberty early are tall compared to other children of their age, but stop growing earlier too, resulting in a short final height. This occurs because their bone age (skeletal maturation) is advanced and their bones fuse early. It also results in early reproductive capacity.
Q. Does early puberty lead to early mental maturation?
Early physical changes do not result in early mental maturation, hence the child may be too immature to deal with the changes in their body.
They tend to be treated by others according to their appearance, rather than their actual age. Children who look older than their age are at an increased risk of sexual abuse, hence appropriate precautions should be taken. Encourage your child to discuss with you any worries or concerns that he/she may be having.
Q. How do I explain my child about these changes occurring in their body?
The child may feel embarrassed by the physical effects of puberty. The child should be told that all children experience puberty, but in his/her case it has occurred sooner than usual. He/she should know that these changes in their body are normal and the children should be allowed to participate in their normal activities.
Q. How do I explain to my child about these changes occurring in their body?
The child may feel embarrassed by the physical effects of puberty. The child should be told that all children experience puberty, but in his/her case it has occurred sooner than usual. He/she should know that these changes in their body are normal and the children should be allowed to participate in their normal activities.
Q. How is it diagnosed?
Early puberty is suspected on the basis of the physical examination. Laboratory tests are important to determine which puberty hormones are present, and where they are coming from. These may include X-Ray of the wrist and hand for bone age (skeletal maturation), hormonal tests of the blood involving multiple samples, ultrasonography of the uterus and ovaries and Magnetic Resonance Imaging.
Q. How is it treated?
Medicines are available to slow or stop early puberty. This also improves the growth outcome. Rarely surgery is needed to remove ovarian cysts, or other ongoing sources of puberty hormones.
Q. What Is Delayed Puberty?
If pubertal changes do not occur in a girl by 13 years of age and in a boy by 14 years of age, puberty is considered to be delayed.
Delayed puberty is more common in boys compared to girls.
Q. What Causes Delayed Puberty?
There are several reasons why puberty may be delayed. In boys it could be a pattern of growth and development in the family. This is called constitutional delay (late bloomer).
Q. How do I know if my child is short and needs to see a specialist?
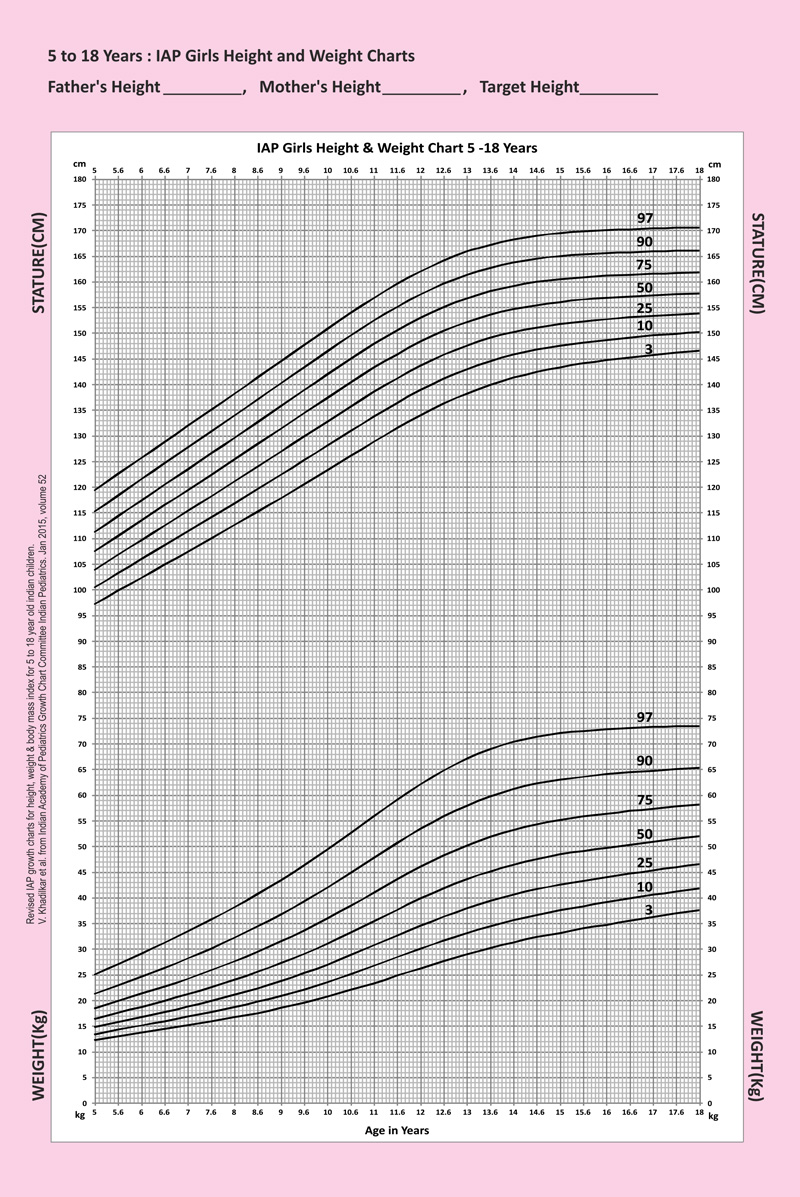
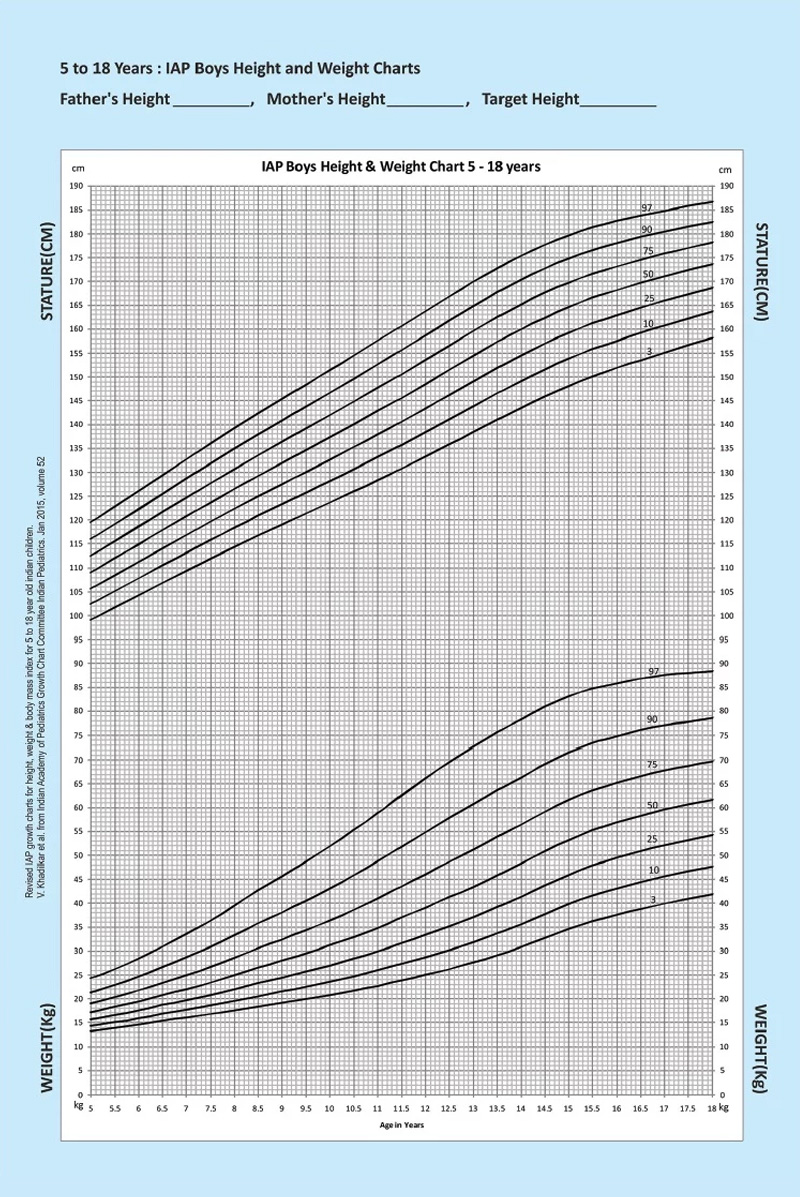
Growth Charts for a population consist of percentile curves which are marked between the 3rd and the 97th percentile. 50th percentile is the average and 3rd and 97th percentile represent the lowest and highest limit of normal.
If you mark the height against the age of the child, and it is below the 3rd percentile (lowest Line), it means that your child is short.
Serial plotting of height measurements on a growth chart is also very important. If your child is crossing growth percentiles in the downward direction, it means that he is not growing well.
View growth chart here
Q. What is Short Stature?
The term Short Stature is used for a child who is below the 3rd percentile when marked on a growth chart for a given population.
Q. When to suspect a growth problem in your child?
A growth problem is suspected if:
- Your baby is abnormally small at birth and has not shown rapid growth after birth
- Your child’s height is below the lower limit of normal on a growth chart
- The child’s height-gain is less than 4 cms per year from the age of 6 years till onset of puberty and less than 6-7cms/year during puberty.
- Your child is crossing percentiles on the growth chart in the downward direction, it means that your child may not be growing normally and needs to be evaluated.
Q. If your child’s height has never been measured, a growth problem may be suspected if:
- Your child is one of the shortest in his/her class
- Your child’s growth over a year has been insignificant
- The child is not outgrowing his/her clothes
- His/her shoe size has not changed for a long time
Q. How do I determine if my child is short because of the parents being short?
Your doctor will measure the height of the parents and calculate the expected height for your child. This is called the mid-parental or target height. Based on this there is a target range for the family.
If your child is short for the family, or not growing well then a number of tests will be done to decide the cause of shortness.
Q. How do I find out the cause of my child’s short height?
Short stature can be genetic or it could be a manifestation of a disease. Your doctor will determine if your child’s height is normal for the family or if he is short. If the child is very short or not gaining adequate height, a series of tests will be done to see if the height is less due to some chronic disease, hypothyroidism, or genetic syndrome. Once all common causes of short stature are ruled out, your child’s growth may be observed for a few months or an evaluation for Growth Hormone Deficiency may be done.
Growth Hormone is a hormone that is essential for growth and a deficiency of this hormone will prevent your child from growing normally. In short girls a blood test called karyotyping may be done to rule out a condition called Turner Syndrome, which is present from birth.
Some of the less common causes of short stature could be:
- Small for gestation (Birth weight <2.5 kgs of a full term baby)
- Genetic defects- Syndromes (Prader Willi, Noonan etc) Skeletal Dysplasias
Your doctor may run some tests to rule out these uncommon conditions if a cause for short height is not found.
Q. How do we test for Growth Hormone Deficiency?
Growth Hormone is a hormone that is secreted by a small gland in the brain called the pituitary gland. It causes an increase in growth through 2 other hormones called the IGF-1 and IGFBP-3.
Growth hormone is secreted in pulses at night during sleep, so a normal child can have a low level if tested.
Growth hormone is secreted in pulses at night during sleep, so a normal child can have a low level if tested.Hence a stimulation test is done to make a diagnosis of growth hormone deficiency. A medicine is given to the child to increase the level of growth hormone and then a small amount of blood is taken every 30 minutes up-to 90-120 minutes. The level of growth hormone is measured in all the samples, and if it less than 10ng/ml, it means that your child may be growth hormone deficient. Along with the stimulation test, the IGF-1 and IGFBP-3 levels are also tested to confirm the diagnosis.
Q. What kind of treatment is given to short children?
All short children may not need to be treated.
If an underlying disease is found, the cause needs to be treated and the child will grow normally
Growth Hormone has been tested for multiple causes of short stature but has been found to be beneficial in increasing the final height only in the following conditions:
- Growth Hormone Deficiency
- Turner Syndrome
- SHOX deficiency
- Chronic Renal Failure
- Small for gestation
- Prader-Willi Syndrome
- Idiopathic short stature
Q. When should a person visit the doctor?
You should visit your doctor or a Pediatric Endocrinologist whenever you observe that your child is short or not gaining height normally. The doctor also needs an observation period to see if the child is growing well and if any intervention is needed, the younger the child, the better the response to treatment. If one keeps waiting till puberty hoping that the child will grow on his own, very often it is too late to improve the child’s height.
IAP - Height & Weight chart
Girls (5 to 18 Years)
Boys (5 to 18 Years)
Q. What is Congenital Adrenal Hyperplasia?
Congenital adrenal hyperplasia is a genetic condition that results from an abnormality of the adrenal glands.
Q.What are adrenal glands and what is their function?
The adrenal glands are a pair of small glands situated above the kidneys. This gland has 2 parts, an outer cortex, and an inner medulla. The medulla of the adrenal gland makes adrenaline. This part is not affected in CAH and remains normal. The outer portion produces three hormones:
1. Cortisol (Hydrocortisone) Cortisol helps to maintain blood sugar in our body. It is also called the “stress hormone” of our body since its production increases during physical stress such as infection and emotional stress, to protect our body. This hormone is essential for life.
2. Aldosterone (salt retaining hormone) Aldosterone is a salt-retaining hormone. It works on the kidneys to help the body maintain normal levels of the minerals, sodium and potassium. Normal levels of sodium and potassium are necessary for all cells to work normally. Deficiency of this hormone results in loss of salt and water in the urine leading to salt deficiency and dehydration.
3. Androgen (male sex hormone) The adrenals of both girls and boys make several types of male-like hormones. These are normally present in very small amounts in children.
Q. What is the abnormality in CAH?
The hormones produced by the adrenal glands are made in a series of steps or chemical reactions.
If one enzyme in this series of chemical reactions is missing, the commonest being 21 hydroxylase, there is a decrease in the end product cortisol and increase in adrenal androgens, which form a part of the series of chemical reactions. The androgens that are increased are 17α(OH) progesterone, Androstenedione, DHEA, and testosterone.
Q. What are the effects of deficiency of 21 hydroxylase
Deficiency of 21 hydroxylase results in :
- Deficiency of the end product, cortisol, which is the stress hormone in our body, and this can be life threatening. It also results in a compensatory increase of a hormone called ACTH that is secreted from the pituitary gland in the brain. Excess of ACTH in the body results in darkening of the skin.
- Increase in the adrenal androgens: These androgens have a masculinizing effect in females. These girls may look like males at birth because the clitoris is enlarged and looks like the penis. The internal structures like the uterus and ovaries are normal in these girls.
- Excessive male hormone in boys results in early sexual hair, acne and increase in the penile size. Due to increase in these androgens, boys and girls have a growth rate that is too rapid. They look much taller than their peers. These androgens also affect the growth plates of children. The bone age is advanced and there is early fusion of the growth plates resulting in short adult height.
- As adults, if the treatment for CAH is not taken regularly, it can cause irregular periods and hair in unwanted areas (face, breast, tummy) in girls and can cause fertility problems in boys.
- Decrease of aldosterone is present in 75% children with CAH. These are called “salt losers”. This results in increased loss of sodium in urine. They develop low sodium and high potassium levels in the blood. These babies do not gain weight, and develop vomiting in the first few days of life. If treatment is not started immediately, it can be life threatening, hence this condition needs immediate attention.
Q. How is CAH treated?
Treatment for CAH should be instituted as early as possible. Treatment consists of replacing the missing hormone cortisol. There are various preparations available in the market, but hydrocortisone is the most preferable. This is available in tablet form in India. The dose of the medication changes with age and regular monitoring by your pediatric endocrinologist with certain lab tests is important for optimal growth of the child. The dose needs to be increased during stress such as infections, fever etc. to cope with the stress.
This medication also decreases the adrenal androgens and prevents further increase in the size of the clitoris in females, early appearance of sexual hair and rapid advancement of growth and bone age. The clitoris may not return completely to normal size, however, and the vaginal opening may remain closed because of the joined labial folds. Surgery may be needed in girls who have a marked male-like appearance of their external genitals. The age at which surgery is done is determined on an individual basis, depending on the severity of the problem.
In salt losers, a substitute of aldosterone called fludrocortisone is given to prevent loss of sodium from the kidneys. This results in normalization of the sodium and potassium levels. This medication is available in tablet form in India. Extra salt needs to be given in babies who are “salt losers” till they start consuming enough salt in their diet.
Q. Will my child become like other children with the treatment?
- With regular and appropriate dosage of medication , your child with CAH can lead a normal life.
- Girls with CAH (if they take their medications regularly) have no difficulties becoming pregnant or carrying a baby.
- Men who take their medications appropriately have normal fertility.
- There are no known mental deficiencies associated with CAH
Q. Can my next baby also suffer from CAH?
The risk of your next baby developing CAH is 25% (1 in 4). The unborn baby can be tested while in the uterus for CAH. Parents with a baby who is diagnosed with CAH, must consult a genetics specialist before planning the next pregnancy.
Q. What is Diabetes?
All parts of our body are made of cells. These cells need energy so that we can perform various activities like walking, talking, or thinking etc. This energy is derived from sugar.
Diabetes is a disease in which the body is unable to utilize the sugar properly and this results in high blood sugar levels. This may be due to deficiency of a hormone called insulin, which is needed for utilizing the sugar in our body or sometimes the body may stop responding to the insulin in our body. In such cases insulin levels may be raised.
Q. Where does sugar come from?
Sugar comes from the food we eat. After we eat, most of the sugar is changed to a form called glucose. This glucose is taken into the bloodstream and the blood sugar goes up. Sugar cannot go into most of the body’s cells by itself. It needs help to enter the cells and this help is provided by insulin.
Q. Where does Insulin come from?
The pancreas is an organ in the tummy that is present near the liver. The pancreas has special cells called beta cells, which produce insulin. When the blood sugar goes up, the pancreas produces insulin. This insulin goes into the bloodstream and helps to bring the blood sugar to a normal level.
Q. What happens when there is not enough insulin (as in diabetes)?
1. The blood sugar goes up because the sugar cannot go from the bloodstream into the cells, in the absence of insulin.
2. The excess sugar begins to spill over into the urine. As sugar spills into the urine, it draws water from the body, so you have to pass urine more often (polyuria).
3. Since water is being lost from the body because of increased urination, you become very thirsty and drink a lot of water(polydipsia). This is your body’s way of trying to replace all the fluid you are losing from urinating too much.
4. There is weight loss because sugar (calories) is being lost in the urine. The body needs energy for working which comes from sugar and fats. In the absence of insulin the sugar in blood cannot enter the cells, to be used for energy. Hence the body cells use fat for energy.
Q. What are the Types of Diabetes?
There are two types of diabetes. These are called Type 1 and Type 2 diabetes.
Type 1 diabetes is also known as Juvenile or Insulin Dependent Diabetes Mellitus(IDDM). This is the most common form of diabetes in young children. In Type 1 Diabetes Mellitus, the beta cells in the pancreas do not make insulin. The person has to take insulin by injection.
Type 2 or Non-Insulin Dependent Diabetes Mellitus (NIDDM) occurs more often in adults, especially if they are obese, although now more and more young children are also developing this form of diabetes. In persons with Type 2 diabetes mellitus, some of the beta cells still produce insulin. In fact at times they make even more insulin than normal but the body does not respond to the insulin.
People with Type 2 diabetes may be able to
- Improve blood glucose levels with diet and exercise or take tablets to :
- improve their insulin production from the pancreas, or
- improve the action of insulin on the cells.
Sometimes, the person may have to take shots of insulin.
Q. What is the reason for developing Diabetes ?
Type 1 or childhood diabetes occurs because the beta cells in the pancreas stop working. This happens because antibodies that are normally supposed to protect our body by fighting infection are produced against the pancreas. These antibodies treat the pancreas like an enemy and destroy the beta cells. Hence Type 1 diabetes is an autoimmune disease. This may occur because of certain viral infections. It is believed that when one develops a viral infection, the body in an attempt to kill the virus starts making antibodies against its own cells (beta cells) by mistake and destroys the beta cells.
One does not inherit Type 1 diabetes, but inherits the tendency to develop these antibodies. Therefore you may develop it even if nobody else in your family has diabetes. You will seldom find several affected members in a family unlike Type 2 diabetes.
Type 2 diabetes or NIDDM tends to be inherited. One acquires the gene for diabetes from one or both parents just as we inherit the color of our skin, eyes etc. Obese people have a higher risk of developing this type of diabetes because of the poor response to insulin. This type of diabetes tends to run in families and you may find several affected members in a family.
Q. What is the treatment for Diabetes?
The blood sugar is high in both Type 1 and Type 2 diabetes, but the reason for this is different.
Patients with Type 1 diabetes cannot produce their own insulin and hence need to take insulin, which is only available as injections at this time. Along with insulin, patients with Type 1 diabetes need certain dietary restrictions. Since food increases the blood glucose level and exercise lowers the blood glucose level, a balance has to be maintained between the dietary intake and exercise.
Those with Type 2 diabetes can produce their own insulin, although they may need dietary control, physical activity and tablets to improve their insulin production, or to improve the effect of their insulin.